









Health and Population

The quality of public health is a major policy issue in every country, whether developed or developing. Citizens demand that a portion of the taxes they pay be returned to them in government hospitals and clinics staffed by government doctors and nurses, immunizations and protection against epidemics, inexpensive drugs, health insurance, and other public health services. The international community, both public and private, also assigns high priority to improving health conditions in developing countries. Three of the eight UN Millennium Development Goals concern public health challenges.248
Reproductive health policy should be everyone’s concern under the goal of responsible parenthood. It effects whether parents are well-informed in exercising their right to choose among alternative methods of determining family size and their ability to raise children who will become productive citizens.
Good health is also a concern of the business community. Healthy employees are more productive, have lower absenteeism, and cost less for private health care plan premiums. More broadly, healthier children and youth are better able to avail of the benefits of education and participate in and contribute to a modernizing economy.
• Public health issues
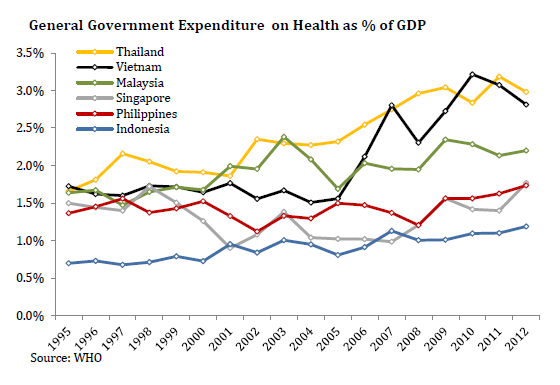
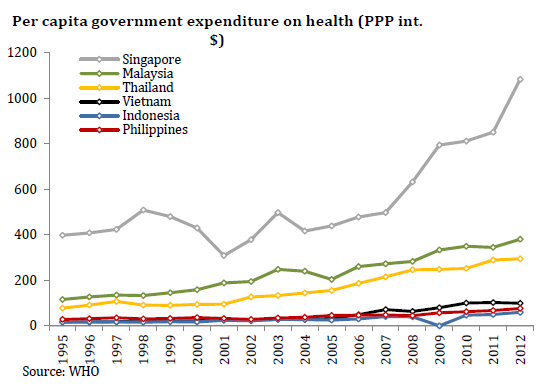
The Philippine national government spent about 1.25% of GDP in 2008 on public health programs in 2008, according to the most recent WHO data (see Figure 247).249 Thailand and Vietnam spent more than 2.5% of GDP, while Indonesia spent less than the Philippines. Although Singapore also spent less as a percent of GDP, it spent the most in per capita terms. Per capita spending in PPP (US$) by the Philippines declined from 2000 to 2008 to be the lowest among the ASEAN-6 (along with Indonesia) (see Figure 248).
China, which is not included in these figures, announced in 2009 a plan to spend US$125 billion over three years to build tens of thousands of clinics and hospitals in order to extend health to almost every citizen.
View original figure here
View related figure here
Figure 248: Per capita government expenditure on health,PPP (US$), ASEAN-6, 1995-2012
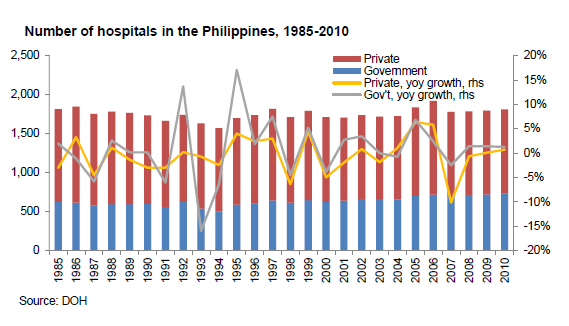
WHO data show the Philippines has 12 doctors per 10,000 persons, 6 dentists, and 61 nurses and midwives. It has often been observed that a sizeable percentage of the population rarely or never sees a health care practitioner. Hospital beds are also scarce with only 5 per 10,000 persons in 2009, compared to 6 in Indonesia, 18 in Malaysia, 22 in Thailand, 28 in Vietnam, and 32 in Singapore. The number of hospitals in the country has barely increased in almost two decades (see Figure 249).
Upper income groups in the Philippines have much better health services than the poor, and there is a concentration of better private sector health care services for this market, especially in Metro Manila and Metro Cebu. An estimated 70% of all health workers are in the private sector. Several new modern hospitals in Manila are among the best in Southeast Asia outside of Singapore. The upper 20-30 percent of the population is able to access these services, but 70-80 million Filipinos are excluded by their low income.
With low government spending on public health and a large population, it is the poorest segment of Philippine society that has the least access to health care services as well as some of the most serious health problems. Examples include:250
• The lifeexpectancy of 70 years at birth is 15 years shorter than in developed countries; for babies born to upper income parents, life expectancy at birth is 80 years, while for the poor it is only 60 years;
• An infantmortality rate of 35 per thousand live births means 80,000 Filipino babies die per year, many being preventable; for high income urban families the rate is 10, while for low income rural families it is 90;
• The maternalmortality rate remains above 150 per 100,000 live births, resulting in over 3,000 mothers dying each year; among higher income mothers the rate is 15 per 100,000;
• Less thanhalf the children from the poorest 10% of homes are immunized, compared to 80% from the wealthiest 10% of homes;
• Mostmedicines are beyond the capacity of most Filipinos to afford; and
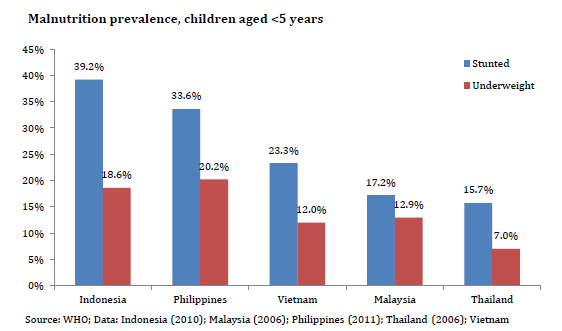
• Malnutrition (weight for age) among young children in the Philippine is much higher than Indonesia, Singapore, Thailand, and Vietnam. Malnutrition (height for age) is not (see Figure 250).
• Universal Health Care (UHC)
Expanding the current Philippine Health Insurance Corporation (PhilHealth) system to provide coverage and services to poor Filipinos and expanding government health care infrastructure to reach deeper into remote areas are two priority objectives of the Aquino Administration. The new Secretary of Health has announced the ambitious goal of achieving UHC within three years.
“We will go beyond ensuring that each Filipino has a Philihealth card. Universal Health Care should mean that every PhilHealth cardholder will get not merely the card; but more important, the essential health services, basic medicines and appropriate quality health cards.”
—Senator Benigno Aquino III, Press Release, Senate of the Philippines, February 19, 2010
The National Health Insurance Act of 1995 (RA 7875), signed in 1995, created PhilHealth, mandating it to provide social health insurance coverage to all Filipinos in 15 years, a goal that has not been achieved. PhilHealth took over responsibility of administering the former Medicare program for government and private sector employees from the GSIS in 1997, from the SSS in 1998, and from the Overseas Workers Welfare Administration (OWWA) in 2005. In 2010 PhilHealth had 20 million registered members.
According to a SWS survey conducted in early 2010 and commissioned by the Pharmaceutical and Healthcare Association of the Philippines (PHAP):
86% of respondents said that the government should provide quality healthcare for everyone, including those who cannot pay;
53% do not have any public or private health insurance;
93% were worried about getting sick, but 67% said they never visited a doctor or health facility for a general check-up when they did not feel sick;
Of respondents who went to doctors at health facilities, 72% said that they paid fees themselves, 16% went to a free or public doctor, 8% used PhilHealth and 5% were helped by family or friends.
To date PhilHealth covers well under half of the population and only pays for hospitalization.251 It provides no out-patient benefits. Membership coverage and benefits have not reached poor Filipinos.
Senator Aquino added that h is administration will strive to improve the local health infrastructure by building “22,000 more barangay health stations, 3000 more outpatient rural health units, and at least 150 more district hospitals.” If elected, he will also increase the health budget to 5%
Senator Benigno Aquino III, Press Release, Senate of the Philippines, February 19
PhilHealth is financed by premiums from the first PhP 30,000 income of salaried employees and a portion of the ACT and EVAT taxes. However, the latter has not been fully remitted to PhilHealth because PhilHealth has accumulated over PhP 100 billion in funds. The current reality of PhilHealth is that the higher income segment of the population receives benefits partially financed by the less fortunate segments of the population, many of who receive no benefits. Persons earning more than PhP 30,000 per month do not pay any premium on their income above that amount. Many professionals do not pay premiums, nor do employers pay premiums for their domestic helpers.
• Population
The debate is intense about whether the Philippines is over-populated and how many people the land and government can support.252 Wealthy Japan, with a similar land area, has a larger population of 128 million, stable and aging due to a low birth rate. But no one believes the Philippines can catch up with Japan economically. Is it moving instead in the direction of Bangladesh and Pakistan, with their populations of 162 million and 170 million, growing at 1.6% and 2.3%, respectively? Probably not, as the Philippine birth rate has been falling, by half over the last three decades. But with over two million births a year and half its population under the age of 21, the Philippines will certainly become more crowded in the decades ahead.
With a population soon to cross the 100 million threshold, the Philippines has overtaken Vietnam to become the world’s 12th most populous country (see Table 86). Within the next two decades, the Philippines could overtake Japan (not growing) or Russia (also not growing) and possibly Mexico (growing at half the rate of the Philippines) and become the world’s 10th or even 9th most populous country.
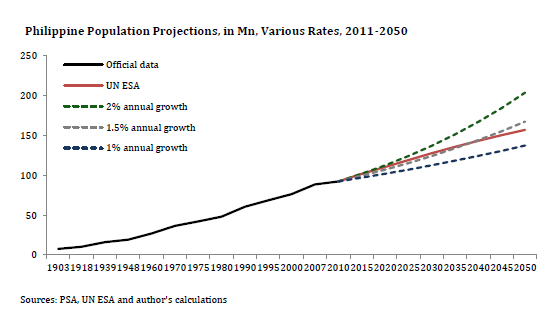
Official estimates show the Philippine population growth rate has slowed from 3.08% between 1960 and 1970 to 2.04% since 2000, a 34% decline, possibly as an effect of rising urbanization, more aggressive campaigns of health advocates, and increased access to information and methods of family planning. However, unless the growth rate continues to slow, the number of Filipinos could double again to 200 million. At a 2% annual growth rate, this would take 35 years. It is more likely, however, to slow gradually. The UN has projected the population to increase over 50% by 2050 to reach 146 million (see Figure 251).
“Thirty years ago, when Noynoy and his family were in exile in Boston, the population of the Philippines was 48 million. It is now an estimated 95 million, and thirty years hence(in 2040) it is projected to reach 140 million”
—Noynoy Takes the Helm in Manila, Paul D. HutchCroft, Director, School of International, Political, and Strategic Studies, ANU College of Asia and Pacific, July 4, 2010

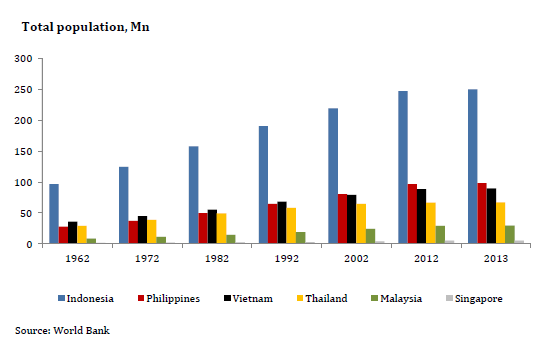
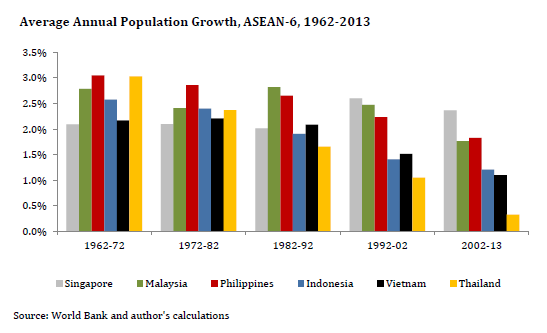
Within the ASEAN-6, the Philippines has overtaken Vietnam to be the second most populous country (see Figure 252). While all the five larger ASEAN-6 countries had population growth rates between 2% and 3% in 1960-1970, by 2001-2009, Indonesia and Vietnam had dropped to 1.5% and Thailand to 1% (see Figure 253).
Since 1960 the population density of all the countries in Table 87 has at least doubled. For the Philippines, it has tripled to 308 persons per square kilometer in 2009. Among the ASEAN-6, the Philippines is higher than Malaysia (84), Indonesia (126), Thailand (132), and Vietnam (268), and lower than Singapore (7,306).

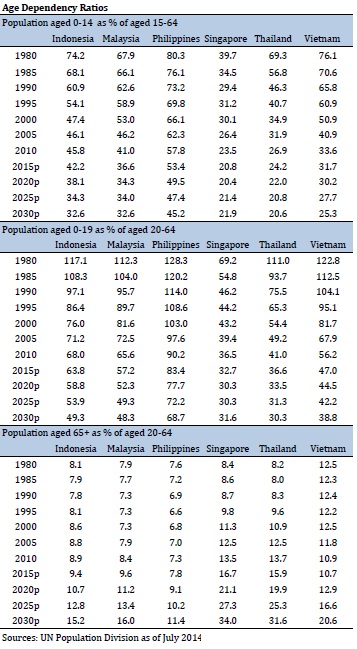
The Philippine population is young, with a significantly higher age-dependency ratio in 2010 than the other five ASEAN-6 economies (see Table 88).
Fertility rates for Asian countries, except for Japan, have been declining since 1960. The Philippines was then one of the highest, at seven births per woman, and almost a half century later remains one of the highest at three births per woman (see Figure 254).

View original figure here
Many Filipino leaders have become increasingly concerned about the negative consequences of the country’s large population. How will the growing population be better fed, kept healthy, educated, and employed? The fertility rate of the poorest Filipino mothers is high because they have little knowledge of or access to family planning. The national average fertility rate is three children per woman but rises to six children for the poorest women. With very low incomes, their families can spend very little for the education and health of each child, perpetuating the cycle of poverty. In developed countries, fertility rates dropped substantially when the state provided social services (healthcare and retirement benefits). In other words, social services have to be improved.
High population growth also affects many investment climate concerns discussed in Arangkada. With four Filipinos born every minute, high population growth creates congestion, requiring accelerated development of infrastructure. Meeting the fiscal demands to satisfy basic needs of a rapidly growing population makes improved governance more critical. Underinvestment in basic education is the major reason most students finish high school unprepared for decent jobs. And the accumulated effects of poverty, congestion, and crime and conflict that rapid population growth exacerbates make security more difficult.
The debate over population policy has intensified with two schools of thought. One argues that the high growth rate must be slowed because the country is overburdened dealing with mass poverty. The second contends that fertility will fall without government interventions, that the population could peak at 110 million in 2025, and that the Philippines must protect its “demographic dividend” and avoid the aging population trend of advanced countries and China.
Some economists point out that no economy has achieved developed economy status with a population growth rate above one percent.253 The Philippines could be in what economists term a low-level equilibrium trap, which “simply means a chain of low economic growth, high unemployment, low productivity, persistent poverty, depleting human capital, and high fertility feeding back into low economic growth, high unemployment, low productivity, persistent poverty, and so on and so forth.”254 If this is true, then lowering the birth rate through a different population policy may break out of the trap, moving the Philippines faster toward developed country status and catching up with the ASEAN-5 economies.
• Reproductive health
The population policy of the national government has for the last decade only advocated birth spacing and natural family planning, while devolving to LGUs all provision of and information about contraception. No national government funds have been earmarked for the purchase of family planning supplies. This policy has been strongly influenced by the Roman Catholic Church. Funding for local government services has been insufficient.
“Poor women face barriers to contraceptive use such as costs, poor-quality services, lack of awareness of or access to a source of contraceptive care, and lack of awareness of methods.”
—Recent study in footnote 3 as quoted by Rina Jimenez David column, Philippine Daily Inquirer, June 5, 2010
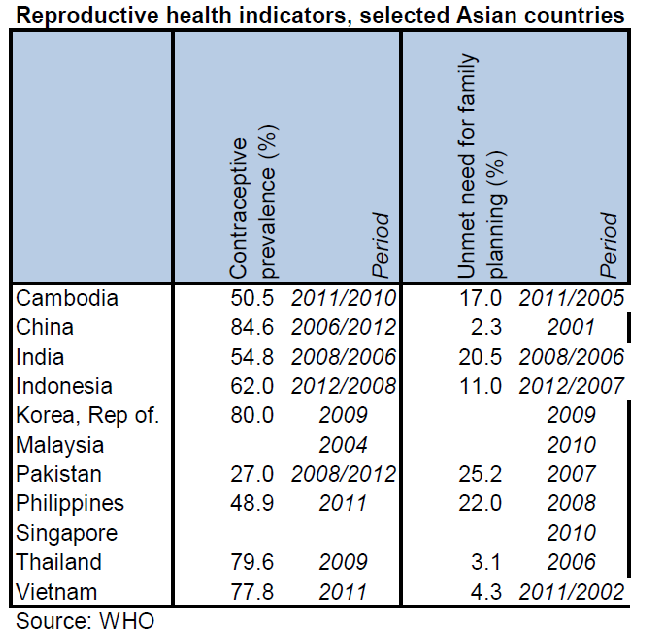
A result of a national policy that does not encourage so-called modern contraceptive methods is a low contraceptive prevalence percentage of 50% and a high unmet need for family planning (see Table 89). The contraceptive prevalence rate appears not to have increased and women of childbearing age want to have two children on average but are having three. Poor women are having two more children than they would like.255
Surveys by Pulse Asia and SWS in 2008 and 2010 also reveal a high level of public desire for a stronger government reproductive health program (see Table 90). For example:
• 82% agreed it is the duty of the government to provide knowledge and materials for modern methods;
• 76% agreed there should be a law requiring government to teach family planning to the youth;
• 44% agreed the government should pass a law specifying the number of children.

Legislation to require human sexuality education in both public and private schools and the government to assist parents with information about and access to contraceptive methods of family planning has been proposed in the Congress for more than a decade. The bill only reached second reading in the House in the 14th Congress. Supporters intend to press for passage early in the 15th Congress.
Comments below on policy show very different views.
• “A strong national family planning program is needed – a program that will not only inform and educate, but instill in everyone a bigger sense of responsibility as parents or would-be parents, and as members of a bigger community. The need is not really to stop population growth, for that would create a different problem altogether, but to slow down population momentum so that in the coming years, the government can be given a chance to provide better services for a manageable number of people.”256
• “Ours is the fourth most crowded place on earth…It is one of the massive weaknesses of the Philippine state – its failure to provide the means for Filipinos to control their lives by being able to choose in the most important decision in a couple’s life, which is having or not having children…We are among the very few countries…whose governments as a matter of policy eschew a population program that provides contraceptives to the poor.”257
• “The Church sees in the bill serious flaws that can lead to violations of human rights and freedom of conscience. It would not be acceptable to pass it in its present form. Total rejection of the bill, however, will not change the status quo of high rates of infant mortality, maternal deaths, and abortions. It is a moral imperative that such dehumanizing conditions should not be allowed to continue. What is needed is a third option: critical and constructive engagement. By working together to amend the objectionable provisions of the bill and retain the provisions that actually improve the lives of the Filipinos, both the proponents and opponents of the bill can make a contribution to protection of the dignity of Filipinos and an improvement of their quality of life.”258
• “We Bishops from all over the country call on President Aquino to listen to the call of the Church that the program of the government to promote a contraceptive mentality through education and medical practices is immoral….”259
• For all couples to achieve their desired family size, contraceptive use rates should increase to be close to those of Indonesia and Vietnam, from the present 50% to 70-80%. A target population growth rate of 1.5% by 2016 would make a huge difference in the future poverty incidence in the country. This can only be done by helping the poor to have fewer children through education, providing appropriate information, and modern method materials. Over time, the number of abortions, estimated at close to 500,000, and the maternal and infant mortality rates should also decline.
President Aquino has expressed his support several times for the right of women to choose their family size and methods of family planning. His administration’s policy is to make available information and materials that would, in effect, reduce the unmet need, increase the contraceptive prevalence rate and reduce the fertility rate, especially of poor women.
The 2011 national government budget for the Department of Health (DOH) proposes an appropriation of PhP 931 million for family health, of which PhP 400 million would be spent on family planning, largely for modern methods of contraception, primarily for birth control pills. Such spending has never been formally proposed nor funded by the national government in the past and has met with objections from senators arguing that it preempts the reproductive health legislation policy debate.
More national government resources and greater public advocacy are needed to help reduce the country’s fertility rate and slow the rate of population increase as soon as possible. The longer the population challenge is not faced squarely, the more extreme poverty will continue and possibly grow.

Headline Recommendations
- Double national spending on healthcare to 2.5-3% of GDP. Direct spending to poorest Filipinos. Government hospitals should be modernized, rationalized, expanded, and many thousands of additional village health centers built. Provide better equipment and staff.
- Expand PhilHealth eventually to become UHC. Include poorest Filipinos at no cost, financed by premiums on higher-income groups.
- Cease misguided healthcare legislation that does not achieve policy goals. Use PPP to encourage private capital to invest in healthcare-related services.
- Government should target an achievable population growth rate, set parallel targets to increase contraception prevalence rate and to lower fertility rate, and design and implement a reproductive health program to achieve targets.
- Congress should pass a consensus version of reproductive health legislation. Private sector should support reproductive health policy legislation and assist employees to have smaller families.
- Government should reward poor families who have fewer children, PhilHealth should introduce a family planning requirement for hospital accreditation.
Recommendations: (9)
A. The Philippine Government should double national spending on healthcare to 2.5-3% of GDP. Direct spending to poorest Filipinos, who cannot afford any healthcare. Government hospitals should be modernized, rationalized, and expanded, and many thousands of additional village health centers built. Better equipment and staff are also needed. (Long-term action DOH, DBM)
B. PhilHealth should be expanded to become Universal Health Care (UHC). Enrollment in Philhealth should be made mandatory so that more professionals, domestics, and informal workers are included. The poorest Filipinos should be enrolled with no co-payments for services required. Outpatient services and free medicines should be added. Premiums should be progressive with income. (Long-term action DOH, DBM)
C. Cease healthcare legislation that does not achieve desired policy goals of improving health of the poorest. The cheaper medicine law has lowered prices for better-off Filipinos, but prices remain out of reach for the poor. Proposed stringent milk code amendments would limit women’s right to choose and do nothing to reduce malnutrition. (Immediate action PLLO, DOH, and Congress)
D. Use the PPP model to improve public sector health services. Opportunities include information technology services (including telemedicine), patient and staff lodging, and air ambulance services. (Medium-term action DOH, NEDA)
E. Government should set a target for an achievable population growth rate (e.g. 1.5% by 2016), set a parallel target for increasing the contraception prevalence rate (e.g. 70% by 2016) and lowering the fertility rate (e.g. to 2.5% by 2016), and design and implement a reproductive health program to achieve the targets. (Immediate DOH, LGUs, and Congress)
F. The private sector should support reproductive health policy legislation and assist employees to have smaller families. The business community should be vocal and visible in the public arena to support government when it acts vigorously to manage population. (Immediate action private sector)
G. Congress should pass a version of the Reproductive Health bill that mandates human sexuality education in schools and provide information and materials for family planning in all government clinics. (Immediate action PLLO, DOH, and Congress)
H. Government should reward poor families who have fewer children, perhaps by adding an amount to monthly CCT payments after the birth of a second child that would be forfeited if a third child is born. (Immediate action DOH and Congress)
I. PhilHealth should introduce a family planning requirement for hospital accreditation. Accredited hospitals would have to make available to parents a full range of legal family planning methods. (Immediate action DOH)
Footnotes
- Goal #4 Reduce child mortality; Goal #5 Improve maternal health; Goal #6 Combat HIV/AIDS, malaria and other diseases[Top]
- Data from the World Health Organization (WHO) includes not just resources channeled through government budgets to providers of health services but also the expenditure on health by parastatals, extrabudgetary entities, and compulsory health insurance payments. It includes resources expended by all these public agencies regardless of source, thus including external donor funding for these agencies.[Top]
- Several of these examples are taken from a presentation in June 2010 Health Equity in the Philippines by former DOH secretary Dr. Alberto Romualdez, dean, Graduate School of Health Science, Pamantasan ng Lungsod ng Maynila.[Top]
- Only 38% are covered according to the National Demographic and Health Survey of 2008.[Top]
- The population of Metro Manila has grown nearly 10 times in 60 years from 1.5 million in 1950 to 14 million in 2010[Top]
- Thurow, Lester, Fortune Favors the Bold, Harper Collins, New York, 2003, p185. “with population growth rates much above one percent, it is essentially impossible to catch up.”[Top]
- Dr. Ernesto Pernia, former head economist, ADB in a paper “Population: Does it Matter?”[Top]
- Facts on Barriers to Contraceptive Use in the Philippines, Guttmacher Institute and health advocacy group Likhaan.[Top]
- MBC research paper on population, January 2004.[Top]
- There are 100 million of us now, Rigoberto Tiglao, PDI, August 12, 2010.[Top]
- Business World column by Jesuit scholar and former Constitutional Convention commissioner Joaquin Bernas, October 19, 2010.[Top]
- Catholic Bishops Conference of the Philippines statement, July 11, 2010.[Top]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}