









Poverty

This section will discuss three important policy areas that affect the business and investment climate. Education determines the quality of tomorrow’s workforce. Health determines fitness of workers. Population determines the numbers of the workforce. The quality of each is extremely important. Well-educated citizens are better qualified for jobs in a modern economy emphasizing knowledge-based services. Good health, aside from being a basic human right, supports increased labor productivity, which in turn supports higher wages. Population policy supports the freedom of parents to choose family size.
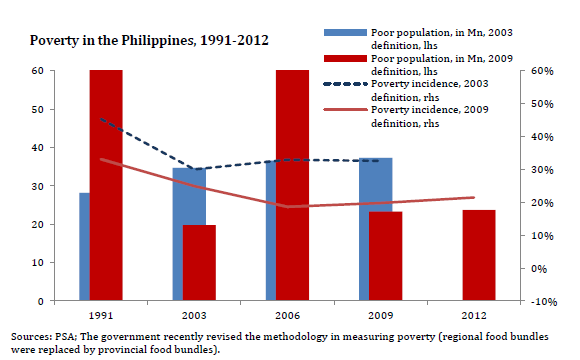
Before discussing each of these policy areas, a look at the statistics of poverty in the country is in order. The latest official survey data is for 2006 (the updated data for 2009 will not be available until 2011). Figure 231 shows the trend over two decades in both the number of poor and poor citizens as a percent of total population. The number of poor declines from 1985 to 1997 from 22.2 million to 18.2 million and then increases to 23.6 in 2006, an increase of 1.4 million over the 1985 level. As a percent of the population, however, there has been progress in a decrease from 41% in 1985 to 28% in 2006.
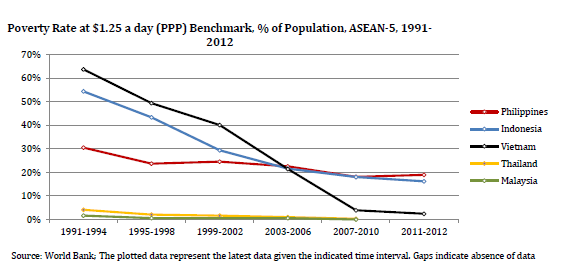
Among the ASEAN-6 the Philippines has the most persistent incidence of poverty (defined as living on less than US$1.25 a day). The other five ASEAN countries have shown steady progress in reducing poverty at this level, but the Philippines, since 1998, has not. By extrapolating the trend direction, the Philippines now has a higher poverty incidence than Vietnam and possibly Indonesia (see Figure 232).
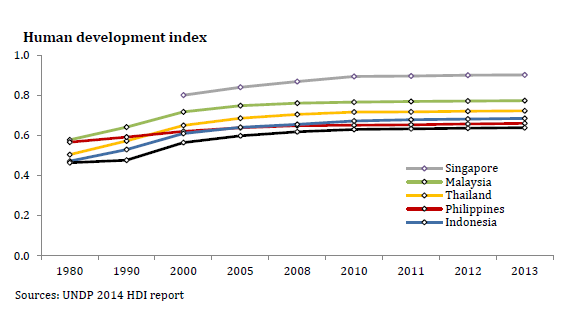
The Human Development Index prepared by the United Nations Development Program (UNDP) measures on the scale of 0.0 to 1.0 (a) life expectancy, (b) education, and (c) per-capita income. While all the countries in Figure 233 below showed improvement, the Philippines was the slowest, ranked with Indonesia and Vietnam in 2007 and lower than the other three ASEAN-6 economies.
View original figure here
A profile of the poor in comparison to all Filipinos is in Table 83. Poor Filipinos are mostly rural, have less access to electricity and water, are mostly farmers, less educated, and have larger families.

View original figure here
View related figure here
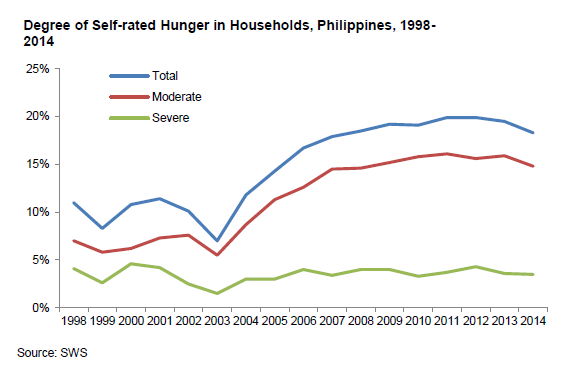
The poor are hungry. Their diet is inadequate. Their children are malnourished (see Part 4 Health and Population). SWS measures self-rated moderate and severe hunger by asking respondents if they have had nothing to eat. The September 2010 poll counted 16% of households – equivalent to some three million families – claiming to have had nothing to eat at least once in the past three months, down from 21% in the previous survey June 2010 (see Figure 234).
 View original figure here
View original figure here
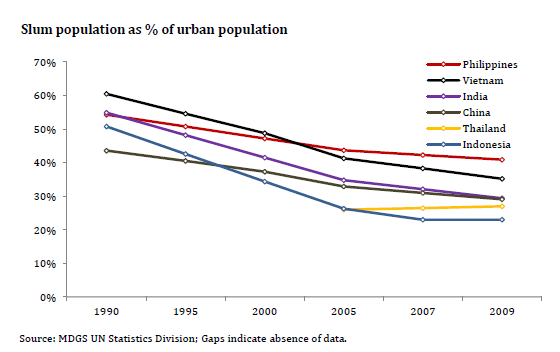
The Philippines has the highest percentage of slum population as a percent of its urban population among six Asian countries. However, most poor Filipinos live in rural areas and migrate to urban slums, where they have better income opportunities than in the countryside (see Figure 235).
 View original figure figure here
View original figure figure hereView related figures here
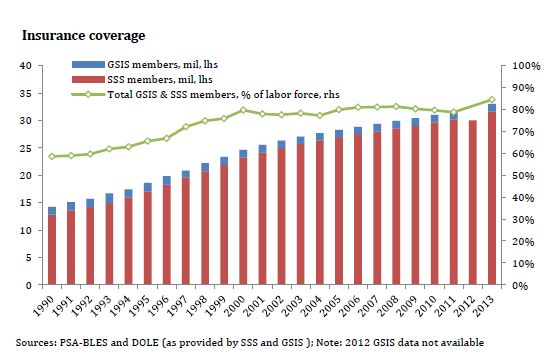
Most Filipinos needing financial assistance approach better-off relatives, who offer better “terms” than banks. Private life and health insurance is not widespread. However, government insurance coverage in the Philippines has gradually expanded to include higher percentages of the total population, as shown in Figures 236. The GSIS and SSS provide retirement payments and loans to public and private sector employees and together cover 80% of the workforce in terms of enrollment. However, the figures for SSS are deceptive. A very large number of persons working in the informal sector (e.g. tricycle drivers) have been enrolled by local politicians in order for them to receive funeral benefits. However, since they do not have regular deductions remitted from their income, they are not entitled to retirement benefits.
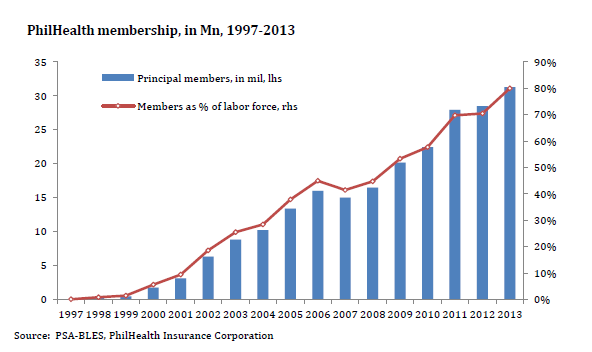
The Philippine Health Insurance Corporation (PhilHealth) membership has grown steadily since 1997, reaching 50% of the labor force in 2008 after a decade of operation (see Figure 237). Expansion of membership continues under the National Household Targeting System, which is currently issuing PhilHealth cards to 800,000 families.
“Of course, the ideal public policy is to provide universal basic health care, when citizens get medical attention based on needs rather than on their income or political color.”
—Benjamin E. Diokno, Will CCT help or hurt the poor?, Business World, October 12, 2010
Benefits from these three programs are very modest by developed country standards. However, the poor, who dominate the informal economy, remain the population cohort still largely excluded from coverage.
 View original figure here
View original figure here
Conditional cash transfers (CCTs) are a new policy instrument in the Philippines intended to improve the lives of the poor, especially children in poor families. They have been used successfully in over 30 countries, beginning in Brazil and Mexico a decade ago. The World Bank in 2009 loaned US$ 2.9 billion for CCT programs in 13 countries, including the Philippines.
CCTs are a social safety net used to incentivize poor families with cash payments for meeting certain requirements that improve the education and health of their children. The intended results are for their children to go to school for a minimum number of days, eat better at school feeding programs, and be healthier. Visits to health center for immunizations and pre- and post-natal care, including counseling for family planning and breastfeeding, are also required. Achieving MDG goals for improved maternal health and reduced infant mortality are supported by CCT programs.
CCTs will not work if the intended government programs are not available to beneficiary parents. Classrooms with teachers and health clinics with health workers must be in place.
The program, which began in 2008 under former president Macapagal-Arroyo, will be expanded by President Aquino to eventually add 4.6 million families (an estimated 23 million persons) by the end of his term in 2016. His first budget included a PhP 21 billion allocation to assist 2.3 million families (an estimated 11.5 million people or one-third of the country’s poor population).
An advantage of the CCT is that the money will reach poor families directly and more efficiently than many past programs that had large leakages, such as benefits going to non-target beneficiaries among political supporters of politicians and the pockets of bureaucrats. Beneficiaries will be carefully selected and their names will be posted on the website of the Department of Social Welfare and Development (DSWD), the implementing agency.
If CCTs are effective in the Philippines, they will reduce school dropout rates (see Part 4 Education) and improve the health of mothers, babies, and children and also will reduce the poverty of the poorest of the poor. In Brazil, along with strong economic growth, CCTs have helped reduce the poverty rate to 15.3% in 2009 from 33.8% 15 years before.
Recommendations: (4)
A. Steadily reduce number of poor and poor as percentage of population. (Medium-term action DSWD, DILG, DTI, DepEd, DOH, DOLE, NEDA, and Congress)
B. Reduce the incidence of hunger. (Medium-term action DSWD, NEDA)
C. Expand insurance coverage to include more poor. (Medium-term action SSS, PhilHealth)
D. Successfully implement the expanded CCT program to include all 6.9 million poor Filipino families. (Long-term action DSWD, DBM)



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}